Creating a single, hard workout is easy.
Creating a series of workouts that improve your overall fitness is not. Creating a true program that builds your skill set, builds your confidence, and adjusts for soreness or an emerging injury is extremely difficult. In the same vein, it is not hard to develop a physical therapy exercise list that targets a single problem, like glute inhibition. It is much harder to progress post-injury using strength training when we need to push the edge of the tissue capacity. Programming a workout needs to consider numerous, modifiable variables. Remember a modifiable variable is anything you can change in the workout to optimize the training session and the overall programming scheme.
At a minimum, you need to consider intensity, sets and reps, rest intervals, frequency of workouts, and supersets.
The minimum however does not optimize your workout and sometimes these are not the most critical or important variables.
If you cannot do a squat without a loss of form, then the most important variable is the one that improves this fundamental movement. If an exercise is not well tolerated (think deadlift causing back tightness or a lunge causing hip pain), then a prep exercise or artificial stabilization may help get the response we want. You can even consider support workouts that can improve an upcoming workout.
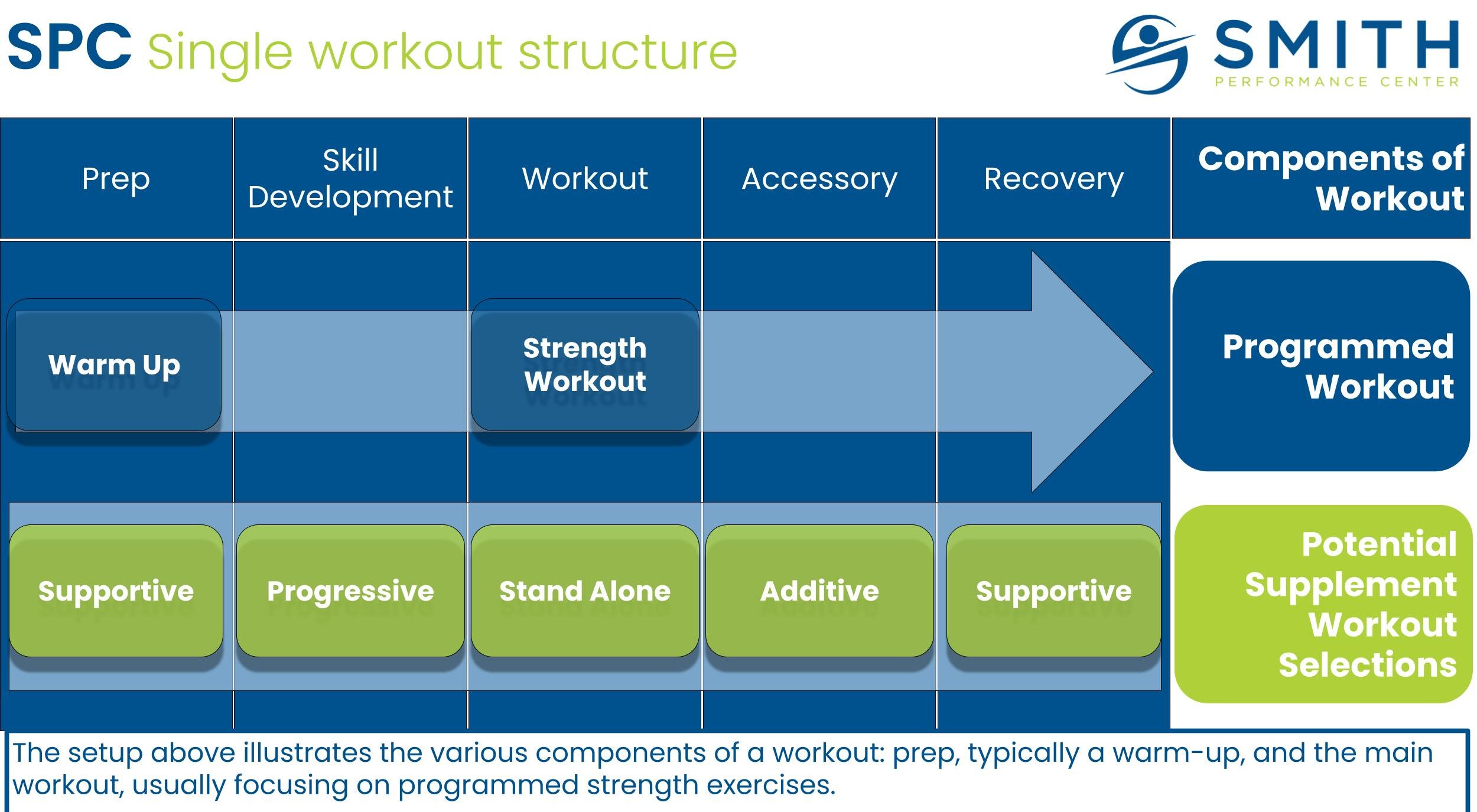
We are going to go deeper into a few modifiable variables that are often not considered that can make or break your success:
- Prep Exercises and PT Additions
- Exercise Choice
- Artificial Stabilization
- Recovery Activity
Prep Exercises and PT Additions
Prep exercises and PT additions are activities that optimize the response to a workout.
Prep exercises are standard activation, stretch, or soft tissue activities in nonpathological areas. PT additions are pathology-based activities that prep the recurrent or chronic injury for activity. For example, let’s imagine that squatting is in your program (We will use the squat as an example to build out a single workout session in the following modifiable variables). A prep exercise may be foam rolling the quads and the thoracic spine during rest intervals. If the squat was painful to the knee because of moderate osteoarthritis, you may traction the knee prior to the squat session which will keep the exercise from provoking your injury. The key for this variable is to monitor the response to a bigger exercise or workout.
If you are someone who feels terrible for the first 10 minutes of a workout, your prep exercises likely stink.
If you hurt during an exercise, PT Additions can make or break your workout.
Exercise Choice
Exercise choice is dependent on how well you move and your experience with it.
A variety of exercises can produce an adaptation as long as it is done correctly. Our bias is to target functional exercises in our movement assessment to understand how well you move and what is the best place to start. If you score low on certain movements, it just means you have a greater coaching need at the start of your exercise program. We do not choose an exercise that you cannot perform.
This sounds basic, however exercise complexity is often ignored and clients overload with an advanced exercise that their body is not ready for.
We can examine the squat again. If you have an issue with transitioning from the descent in the squat to the ascent, we can choose a loaded sit-to-stand to remove the difficult transition phase. We could progress load with the sit-to-stand and eventually progress to a normal squat, depending on our goal of either building overall strength or building movement capacity.
Artificial Stabilization
Artificial stabilization is any tool used to improve the performance or tolerance of an activity.
This concept was developed initially by our physical therapy team to aid in our diagnostic phase. Our strength coaches use artificial stabilization to help with tolerance of progression, volume, and intensity. The most common place we see artificial stabilization is the use of bracing to support heavier lifts, like deadlifts or squats. However, we can use artificial stabilization in many ways.
We want the artificial stabilization to be a training aid, not a crutch.
| Artificial Stabilization | When is it used |
| Modified Low Dye | During running volume increases |
| Thigh strap | During increased load or if abnormal symptoms are noted with load |
| Lumbar brace | During heavier loads |
| SI loc belt | Post-pregnancy or in individuals who are hypermobile during split-leg positions |
Recovery Activity
Recovery is the most underused variable in training.
We often see individuals who have never built in recovery to their programming. Our standard is 4 weeks followed by a recovery week. If you are noting a progressive loss in performance, this would be a good place to start modifying. However, recovery also includes performing activities that make your workout response better.
Here are some examples:
- If you are prone to low back tightness post-workout, traction the lumbar spine after you complete the exercise.
- If you are prone to headaches or neck tightness after shoulder pressing, use a lacrosse ball over the thoracic spine.
- If you experience excessive soreness a day or two after a hard workout, perform activation exercises of the antagonist muscles immediately after your workout is completed.
Optimizing your response to exercise
This may seem obvious, but feeling terrible after exercise is not good.
These modifiable training variables can be used just as systematically as the more common sets, reps, and intensity. If you are feeling rough after workouts, noting more tightness or cramping, then you will benefit from using these variables to improve your response to the workout.
Do you struggle with maintaining an exercise routine?
Let us help you develop an exercise routine that can work even with a busy schedule.