Cramping is at the top of the list of common problems that we think are misdiagnosed and mismanaged.
Watch the following video to learn more!
Recurring injuries derailed Alex’s triathlon training for years—until he adopted a structured, phase-based rehab approach. This case study shows how the Smith Performance Center Phase System helped him move from chronic pain to consistent performance by focusing on what most athletes overlook: building tissue capacity to match training demands.
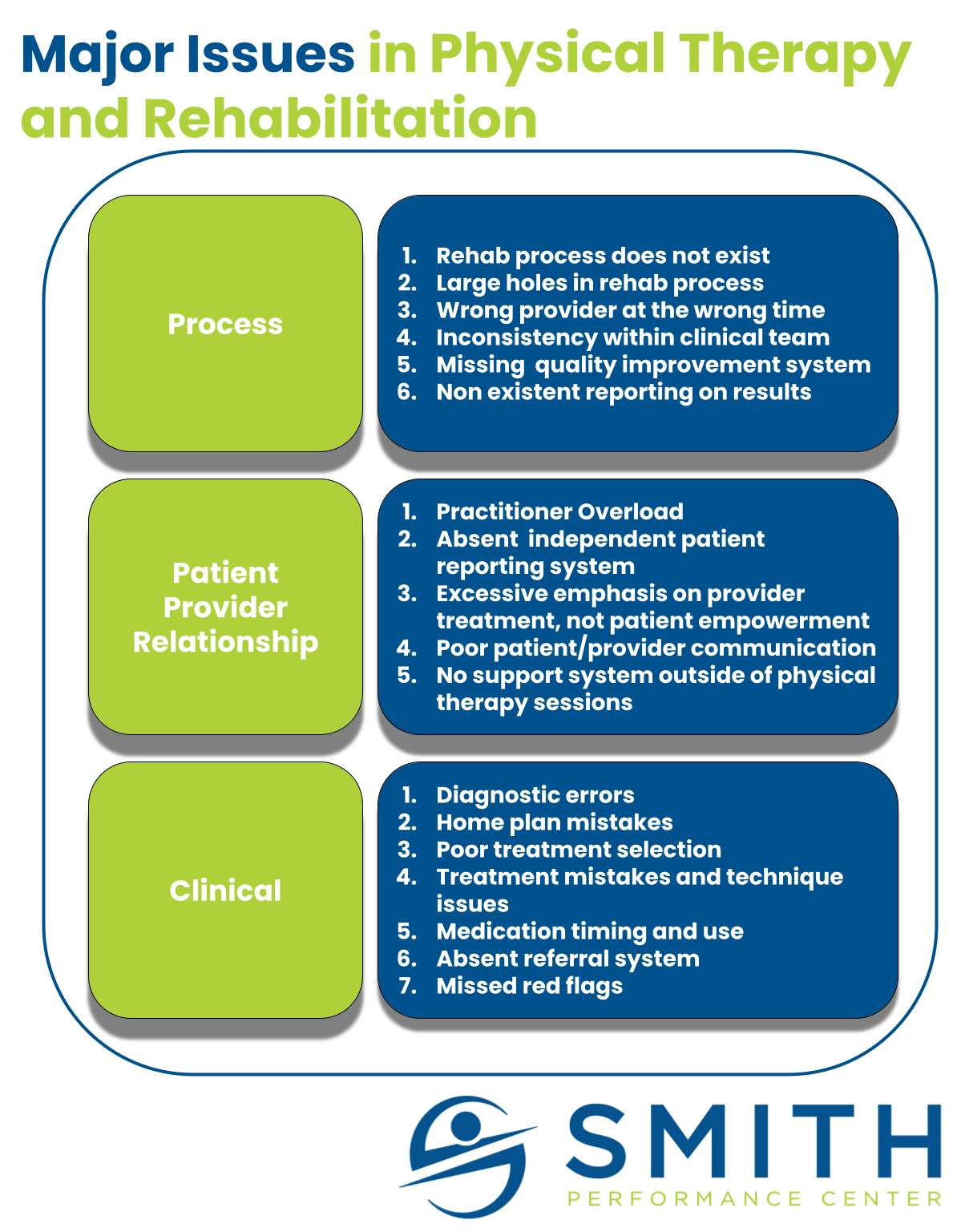
Physical therapy quality is highly inconsistent between clinicians, clinics, and companies. Numerous factors play into these discrepancies, including clinical process, management structure, payment models, clinician-patient time, use of assistants, patient load, clinician training, and business models. These issues often culminate in underwhelming rehabilitation outcomes for clients. When embarking on a rehab journey, most patients don’t anticipate these issues. As Sarah Smith, PT, DPT, and co-founder of Smith Performance Center, observes: “Many patients don’t know where to start their rehab journey, and physical therapy is often not their first choice.” Choosing a clinic that treats 25 patients daily with heavy use of assistants is vastly different from one that sees six patients daily with dedicated one-on-one time. Blending the art and the science of physical therapy requires more than most patients realize. From our experience, three key areas drive these differences: Process, Patient-Provider Relationship, and Clinical Skill. Clinics that avoid assistant
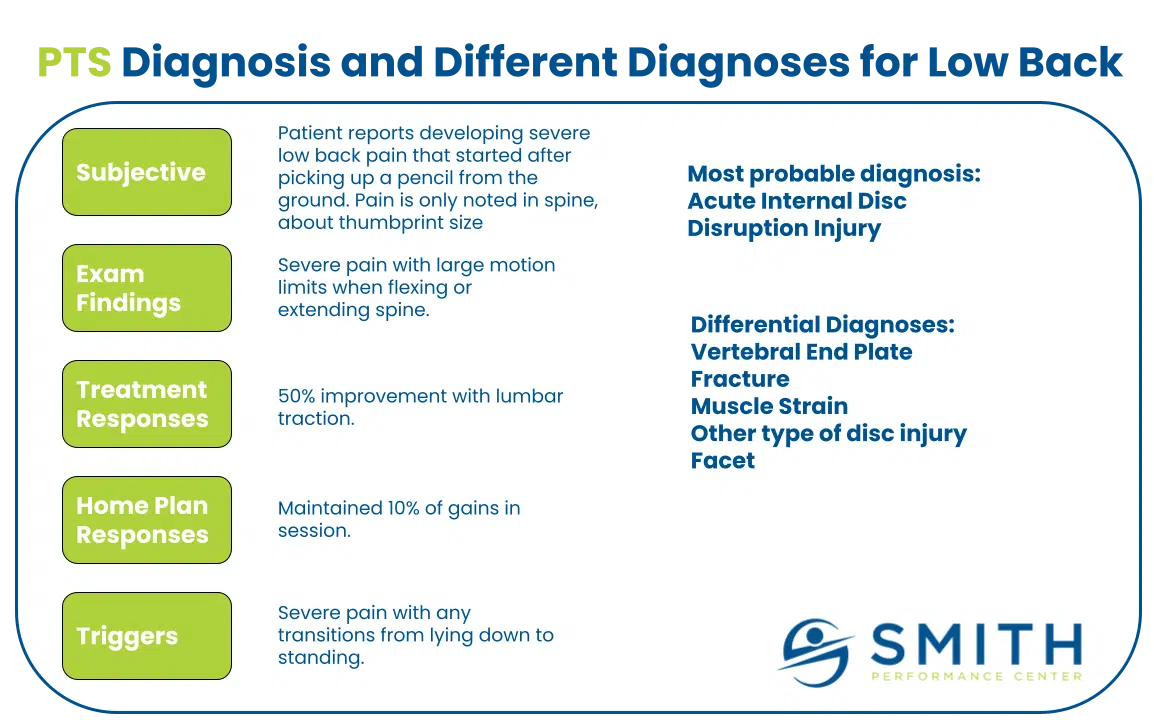
“My butt hurts.” A significant proportion of my conversations start with this statement. She continued, “ I have regular active release along with dry needling. I stretch my hamstring ALL THE TIME and I still have pain.” Her frustration was palpable. “I know I have a tight hamstring and there is scar tissue. But it’s been 8 months.” She assumes the pain must be the hamstring; we call this the pain generator. The hamstring tendon attaches right where her pain starts. The tightness is over the hamstring muscle belly. She describes the pain in a clear way that implicates the hamstring. She made a convincing argument that the hamstring is the issue and the diagnosis has been repeated by multiple medical providers including a physician and two physical therapists. The location matched. Running increased the pain. Another match. Stretching and manual therapy provided temporary relief. But 8 months into the
Recurring injuries derailed Alex’s triathlon training for years—until he adopted a structured, phase-based rehab approach. This case study shows how the Smith Performance Center Phase System helped him move from chronic pain to consistent performance by focusing on what most athletes overlook: building tissue capacity to match training demands.
Physical therapy quality is highly inconsistent between clinicians, clinics, and companies. Numerous factors play into these discrepancies, including clinical process, management structure, payment models, clinician-patient time, use of assistants, patient load, clinician training, and business models. These issues often culminate in underwhelming rehabilitation outcomes for clients. When embarking on a rehab journey, most patients don’t anticipate these issues. As Sarah Smith, PT, DPT, and co-founder of Smith Performance Center, observes: “Many patients don’t know where to start their rehab journey, and physical therapy is often not their first choice.” Choosing a clinic that treats 25 patients daily with heavy use of assistants is vastly different from one that sees six patients daily with dedicated one-on-one time. Blending the art and the science of physical therapy requires more than most patients realize. From our experience, three key areas drive these differences: Process, Patient-Provider Relationship, and Clinical Skill. Clinics that avoid assistant
“My butt hurts.” A significant proportion of my conversations start with this statement. She continued, “ I have regular active release along with dry needling. I stretch my hamstring ALL THE TIME and I still have pain.” Her frustration was palpable. “I know I have a tight hamstring and there is scar tissue. But it’s been 8 months.” She assumes the pain must be the hamstring; we call this the pain generator. The hamstring tendon attaches right where her pain starts. The tightness is over the hamstring muscle belly. She describes the pain in a clear way that implicates the hamstring. She made a convincing argument that the hamstring is the issue and the diagnosis has been repeated by multiple medical providers including a physician and two physical therapists. The location matched. Running increased the pain. Another match. Stretching and manual therapy provided temporary relief. But 8 months into the