We treat intractable knee pain on a daily basis.
Our process is called the PT Solutions Treatment Hierarchy. The treatment hierarchy allows our team to support the diagnosis, reduce pain, and create a clear home plan. Building a treatment framework is a critical component of the plan and it changes based on the key sign, the structural diagnosis, and the trigger management plan. For example, a person with an anterior horn meniscus lesion, we would first normalize painful end range extension of the knee. Once passive extension is pain free, we would start to load their leg with the activity that normally hurts, providing them an exercise like terminal knee extension with the band that will keep their knee extension pain free. Finally we would dig through all of their daily activities that cause symptoms like fast walking or going downhill and stop them from doing it to allow healing.
We use this type of structure for each injury, focusing on the most effective methods with the least reduction in activity.
5 treatment options for knee pain
When your knee pain does not go away, you may find yourself digging through article after article on google.
Remember there is not a one size fits all exercise for each injury and there an infinite number of things to try. Some will help and some will not. Our process focuses on what works and amplifying it. We use a treatment hierarchy.
Treatment Hierarchy
- Tissue specific treatment like manual therapy to the painful joint or tissue
- Artificial support, bracing, taping or training aids to reduce load, change patterns, or replicate muscle force
- Activation and inhibition exercises
- Targeting relative stiffness or laxity in the kinetic chain
- Movement retraining
The test retest methodology to capture the biggest response in session. The test is called our key sign. The key sign allows us to perform a treatment and then go back to the key sign to determine if it gets better or worse. A key sign can be a finding in the exam or an activity that a patient can perform that causes the pain. The easier a key sign is test the more effective we can be. Walking that is immediately painful is a great key sign to test. Pain first thing in the morning is not a great key sign because we can’t do it at the session and would need to wait until the next day to see if treatment works. We want a fast feedback loop.
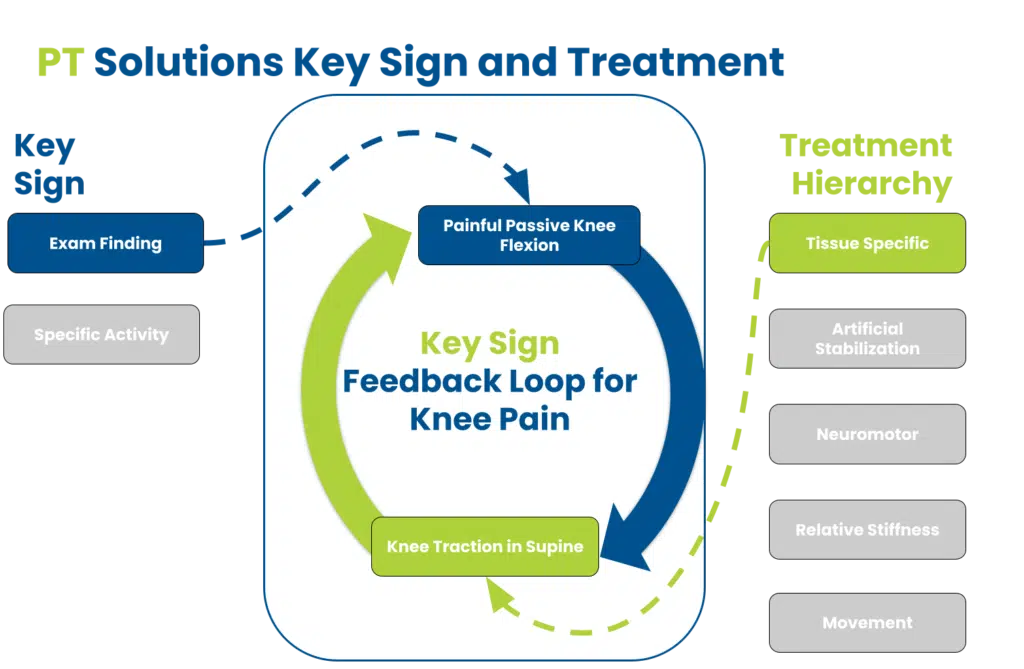
If a change occurs, then we know there is a treatment we can leverage to help you.
Tissue Specific Treatment
When we describe tissue specific treatment, we mean the tissue that is causing the pain.
The pain generator can be from the patellar tendon, quad tendon, the patella, meniscus, ligament, the tibiofemoral joint, the patellofemoral joint, the extensor mechanism, the quad or hamstring muscle, bone, nerve, referral from the hip or low back, or due to scars from an injury or after a surgery. Figuring out which one of these is the culprit is always the first step of the process. You can read more about our diagnostic process here.
Lets consider two very common pain generators: the joint and the meniscus.
Joint Pain
The most effective treatment we use for the ‘jammed’ joint is traction.
Click here to see our videos on partner and self traction. Traction can regain motion, reduce pain, and start to improve gait.
Meniscus Injury
When the meniscus is compromised, the smooth operation of moving out of the way of the two long bones doesn’t seem to work as well. The most effective treatment involves regaining passive motion with manual therapy like mobs. You can also follow it up with an exercise like terminal knee extension if the pinch is happening at the front of the knee.
Artificial Support-Unloading the painful knee
The artificial support portion in our treatment hierarchy is the most commonly misunderstood; the artificial support is not permanent.
For example, using a cane is very effective for knee pain where motion is lost and the joint has swelled. Since we walk so well it can seem like there is minimal load to the knee. This is not true. There is tremendous load to the knee during walking and normal movement. The single point cane used in the opposite hand reduced the knee abduction moment that occurs at midstance (the middle of stance phase where you are effectively balancing on one leg). When we give this medical advice, patients will push back because of the stigma associated with using a cane, but if you reframe it as a short term tool let the knee feel better, you can save yourself a lot of pain.
Another unloading strategy is to brace the lower extremity for patellofemoral pain, the SERF strap can replicate the gluteus medius action to control hip motion. This reduces stress and load to the knee. Often it resolves the pain that is being driven by the abnormal loading strategy.
Activation and Inhibition Exercises
The traditional knee exercises that you see on YouTube or get primarily at other clinics are activation or strengthening exercises.
For our physical therapists, actual weakness is less common that inhibition.
Inhibition happens when something makes it difficult for a muscle to fire. Typically this occurs from swelling (effusion) in the knee capsule. Remember there is not a perfect knee exercise that solves each presentation of knee pain. There are numerous knee exercises to choose from, but I will use straight leg raises as an example as it is often prescribed even when it is not the right exercise at the moment. Straight leg raises require you to keep the leg completely straight and lift one leg up from the table while the other stays down. The quad is asked to flex the hip via the rectus femoris with support from the other hip flexors while the knee does not bend. If the knee bends, we call it an extensor lag. Complete knee extension should be present or this exercise can actually cause pain.
A better exercise would be the long arc quad in pain free range of motion.
You could also do terminal knee extension exercise with the band which would help strengthen the quad while helping the rolling and glide mechanics of the tibia and femur. Once full extension is achieved, we could add the straight leg raises into the home plan.
Relative stiffness in the kinetic chain
If you consider movement in the entire whole, there will be parts of the body that are easier to get motion and some that are harder.
This means that your body will start with the area that is easier to get motion first. If you have a motion limitation in the ankle, the knee will get more stressed. If hip extension is limited, you will get more stress at the low back or the knee. Here the idea is that we do not forget the impact of other areas of the body on the knee. BUT we do not start here.
We believe treating the painful tissue first will often help with relative stiffness issues.
Movement Retraining
Movement retraining is needed in some cases.
This can happen due to a variety of reasons. There are two big ones that I want to consider: walking and running.
Walking
The load to the knee joint with walking is significantly more than you think. The knee joint goes into full knee extension at least two times. This does not happen with running and sometimes means that people can run without knee pain but have issues with walking. Once the knee is traumatized and swollen, the ability of the quad to fire is compromised.
The quad inhibition leads to less force absorption and more trauma to the joint itself. When you watch someone with a swollen (also known as effusion) knee walk, the joint will appear to stay straight the entire time. This is not good and means the quad cannot handle the load of walking. So without conscious thought, you will start to walk with a straight leg.As a general rule, if you have swelling then you must active the quad muscle with an knee exercise like long arc quads any time you stand up and start to move. Our physical therapists will recommend this even if walking is pain free.
If walking is actually painful, we highly recommend the single point cane to make walking pain free.
If the change persists, then we will break your walking gait down and retrain it.
Running
Running leads to much larger forces than walking. It is more complicated than the often repeated statement that you have glute weakness. A running analysis must look at more than form and glute strength. There can be a variety of issues including strength, motor control and sensory impairments.
Each of factor can lead to pain and overload at the knee joint. For example, the quadriceps can be fully maxed out in running while walking typically hits around 40% of the maximal muscle contraction.
Like walking, we will see quad inhibition from joint swelling. Since the quad will be fully loaded with running which does not happen in walking, a straight leg gait pattern is very common. This happens when the body does not trust the quad to absorb the force. Instead you transfer the force right though the joint. The result is a spiral of joint swelling leading to less quad strength leading to more joint loading and then more swelling. We call this the doom loop.
You can see more on this in a review of differentials for running downhill.