‘Not all relevant outcomes can be assessed with a device, a laboratory test, a physical finding or some other data gathering independent of the patient’s perception and voice.’
-Kroenke, Monahan, and Kean 2016
We want to share with you how filling out patient forms is not only useful to our team but also critical for receiving the best care.
In the ranking of where you want to spend your time, completing forms for a medical visit is just above a tooth extraction. The act is mind-numbing. Partially due to the perceived lack of benefit and partially because you know the healthcare provider isn’t using it. They will even ask the same questions that were already answered in the form.
Our team would like to change your mind on this by showing how we use your forms to impact your care – the why, how, and when.
There are three clear information channels that our practice can monitor: provider experience, patient experience, and admin experience.
The provider documentation is expansive and includes 4 main areas: subjective, objective, assessment, and plan. This information is required to practice and details what the provider is hearing, seeing, and thinking. The admin experience is about the stuff outside of the session – scheduling, billing, and communication. This is often over the phone or via email without practice admin. The patient experience can only be captured in the forms you fill out. Remember that while the healthcare provider is writing down what you say, it’s through the lens of the provider.
This is one of the most critical aspects of patient forms – providing a realistic view of what you feel is happening which may contradict what the provider is perceiving.
The patient experience is critical to document and systematically record. As the quote above elucidates, not all relevant information can be captured in an exam. But a free for all, writing whatever you experience, is also not helpful due to poor interpretation and increased time needed on the part of the patient.
This means we need structured forms and entries to reduce the time for you to fill out, less mental stress on the provider to interpret, and standardization for quality improvement.

The 4 reasons your responses matter
There are four primary reasons to track the patient experience:
- There is no replacement measurement for what you are experiencing
- Actionable information for treatment while reducing provider bias in your responses
- Allows for comparison between patients
- Improves reporting to providers on what works, what does not, and when
There is no replacement measurement for what you are experiencing
We cannot read your mind…yet.
This means we need your input to tell us what is happening. Here is a common issue, your exam will improve as will your performance on an activity. Occasionally this results in you saying ‘I feel better.’ But this also results in you doing more which can often lead to your pain remaining the exact same or even getting worse.
There is progression but there is also an issue that needs to be addressed.
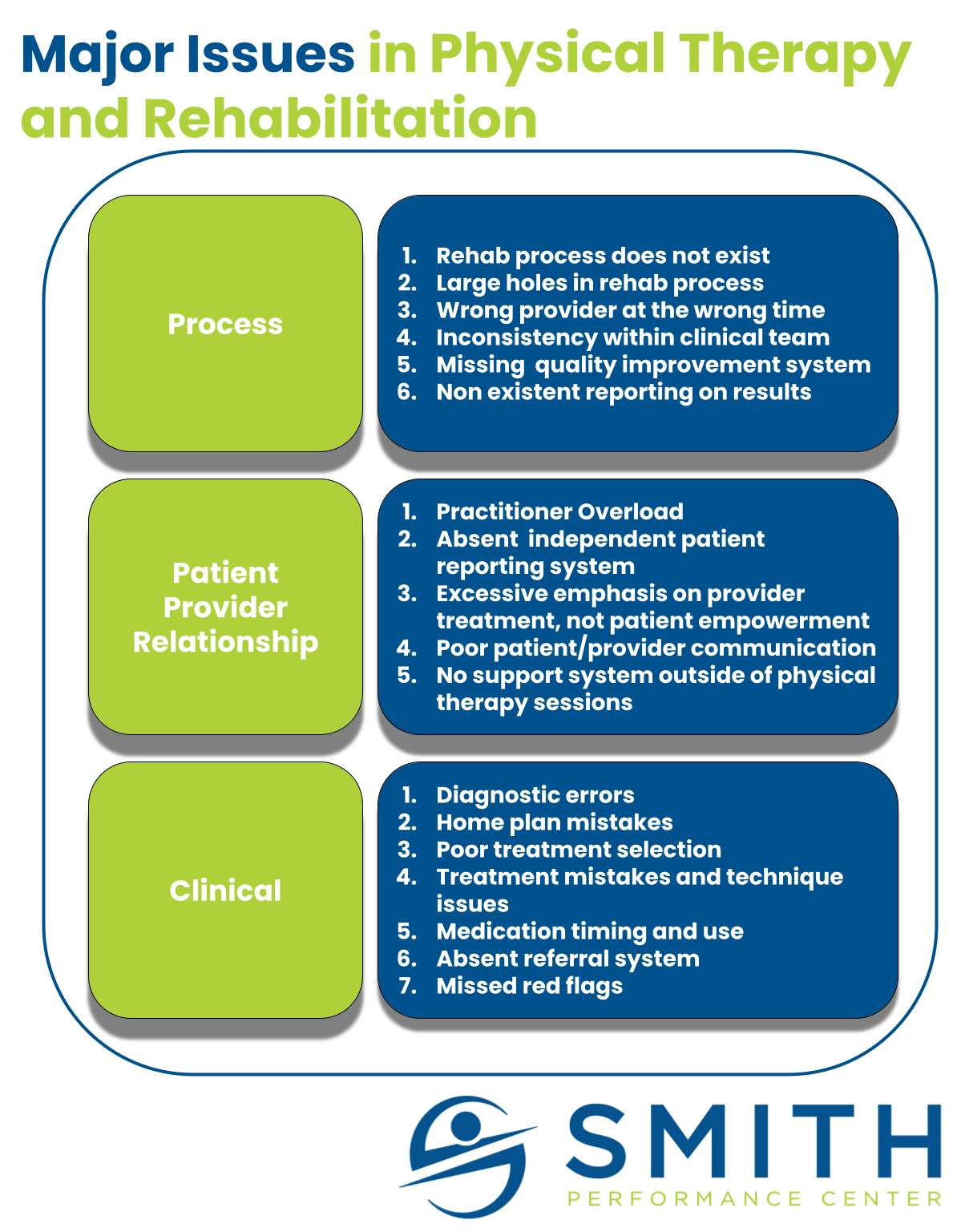
Reliance solely on the provider will not solve every solution and critical aspects of the rehab process will be skipped.
Actionable information for treatment while reducing provider bias in your responses
The patient forms directly impact our focus on what is the most important problem to solve.
Our team has a rehab process beginning at diagnosis and going till you no longer need us. If you tell us that there is no improvement in the session, then we know we are still in the diagnostic phase. This means we do not have the right diagnosis or pain management strategy in place. However if you have a great response in session with complete pain relief and then we see on your pre-session form a week later that you lost all of the progress, we know that your home plan or symptom stabilization is the issue.
The response is critical and helps us actually determine the structure of your visit.
Allows for comparison between patients
Our team has treated thousands of patients.
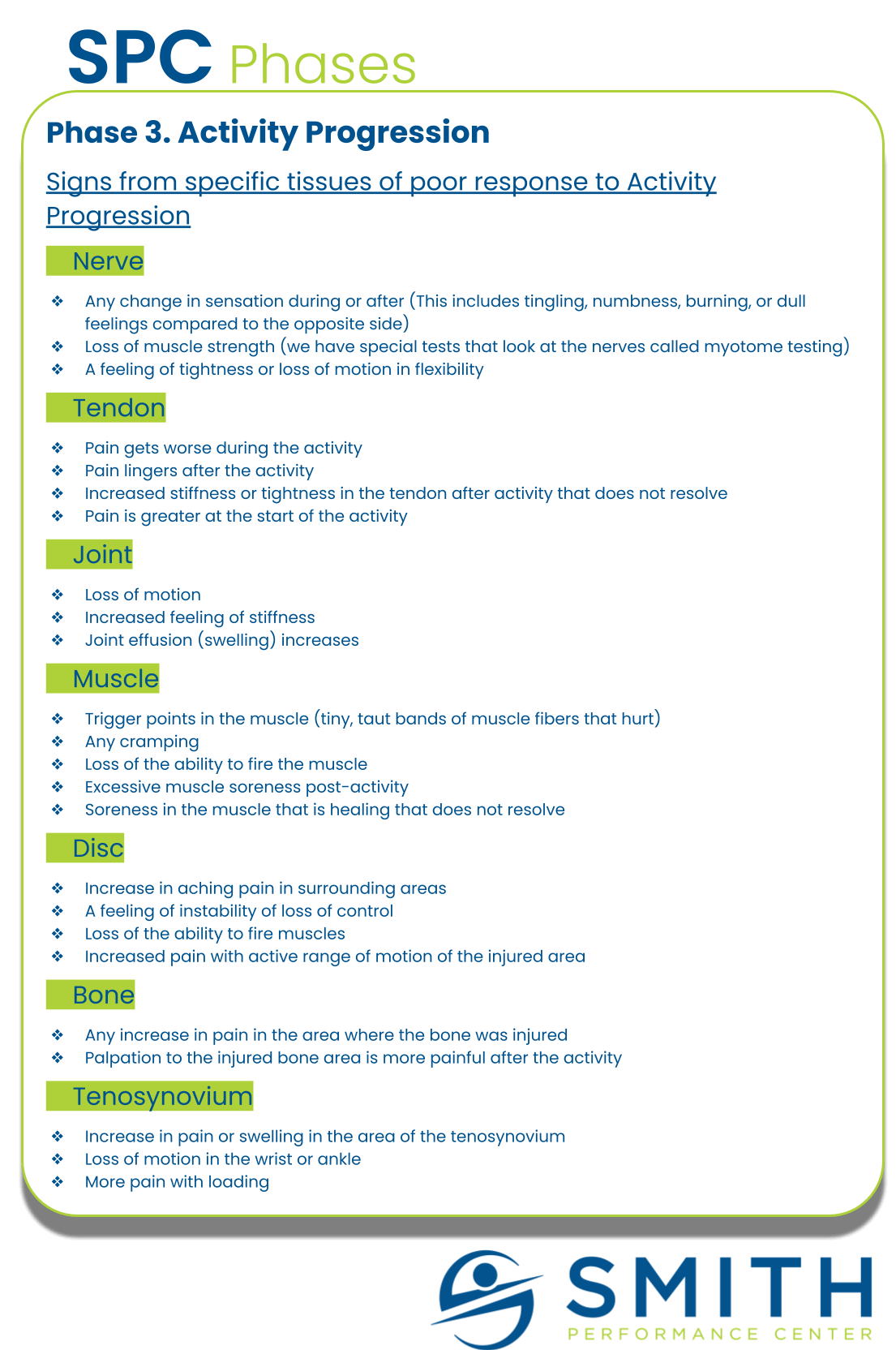
The more information we capture, the more patterns we can uncover. For example, we can see that starting knee traction with a leg weight too early in the symptom stabilization phase can actually cause more setbacks. We can see that partner support by using manual therapy we teach can drastically reduce the visits you need at our clinic. We can see that activity progression works well with the support of our coaches but we still need physical therapists involved to manage new issues or stabilize flare-ups.
Capturing your information allows us to see what has worked in similar patients and to use it more while eliminating things that make patients worse.
Improves reporting to providers on what works, what does not, and when
At the most basic level, the ultimate success of our service depends on what you are experiencing, from start to finish.
We want to have results that improve in sessions, between sessions, in one month, and by the time of discharge. Our goal is fewer visits with better results. This takes incredible amounts of information and work outside of the actual sessions. Without this information, we cannot be certain we are helping. We cannot call ourselves experts. We cannot get honest feedback.
Your responses help us get better and serve future patients better.
We appreciate your help.