Physical Therapy Research
The connection between your knee, an injury, and the brain is not straightforward. However, when you hurt your knee or any other joint there can be issues that lead to future problems. A recent article dove into this topic:
Grooms D, Appelbaum G, Onate J. Neuroplasticity following anterior cruciate ligament injury: a framework for visual-motor training approaches in rehabilitation. J Orthop Sports Phys Ther. 2015;45(5):381-393.
Why is this important for physical therapy?
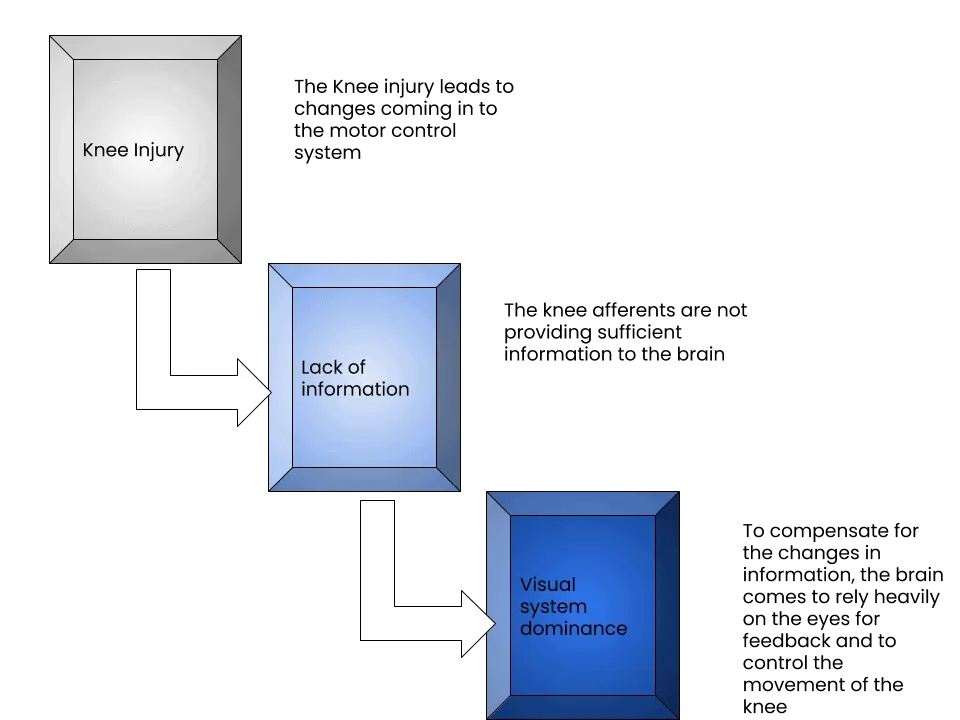
The control of our body is dependent on three systems: visual, vestibular, and somatosensory. The visual system contribution is obvious – the eyes. Due to changes in information coming from the body (somatosensory) due to the ACL tear, the motor control system becomes more reliant on the eyes. If we focus on retraining the body without disrupting this natural progression to visual dominance, the athlete will be at risk for injury as they progress to more demanding activities. Well-designed return-to-play programs follow a task-based outline for progression. As the athlete progresses from a closed environment with simple tasks, the use of visual feedback is not a problem. However, the move into an open environment with this strategy requires more motor planning on the part of the athlete. A complex open environment (like playing soccer or basketball against other players) leads to huge demands on the brain as it attempts to use vision and a top-down approach to control the knee. This is a large cognitive load that appears to eventually fail as seen by the injury rates.
What is the research saying?
During treatment, athletes need to train the somatosensory while blocking the dominance of the visual system. The use of blindfolds and stroboscopic glasses can force the body to use the impaired somatosensory system. As the athlete progresses in rehab, the dominance of the visual system needs to be constantly assessed or visual dominance will develop. The significance of this problem will not be exposed until the athlete is under a large cognitive load (ex. reacting to an opponent while attempting to cut and maintaining control of the ball simultaneously). During the large cognitive load, using the visual system to maintain adequate control of the injury knee will be impaired leading to risky knee behavior.
The following exercises could be included in the physical therapy regimen of an athlete coming off an ACL surgery in the their task-based progression.
Blindfold Single Leg Balance
Blindfold Step Down
Physical Therapy Takeaways
Smith Performance Center uses blindfolds, eyes-closed exercises, and stroboscopic glasses with physical therapy and PT movement knee group. The authors included a photo of exercises that included an athlete performing an exercise while going into knee valgus, which we consider a problem. Since this is a predictor of knee injury, the inclusion of this without a comment was interesting. Understanding the there is a tendency to develop visual dominance for motor control feedback and control of the injured knee could be a game changer. Due to the disruption of the ACL and damage to afferents in the system, it may be impossible to prevent this process from occurring but at the least we need to make changes in the overall plan to account for this problem.
Clinically, we see most knee injuries lead to a poor ability to balance. This is increased with eyes closed. We test any knee injury for this issue as a lack of sensory control at the knee could cause more problems in the future.
Want More? Check out the following articles:
Courtney C, Rine RM, Kroll P. Central somatosensory changes and altered muscle synergies in subjects with anterior cruciate ligament deficiency. Gait & Posture. 2005;22(1):69-74.
Kapreli E, Athanasopoulos S. The anterior cruciate ligament deficiency as a model of brain plasticity. Medical Hypotheses. 2006;67(3):645-650.
Kapreli E, Athanasopoulos S, Gliatis J, et al. Anterior cruciate ligament deficiency causes brain plasticity: a functional MRI study. Am J Sports Med. 2009;37(12):2419-2426.
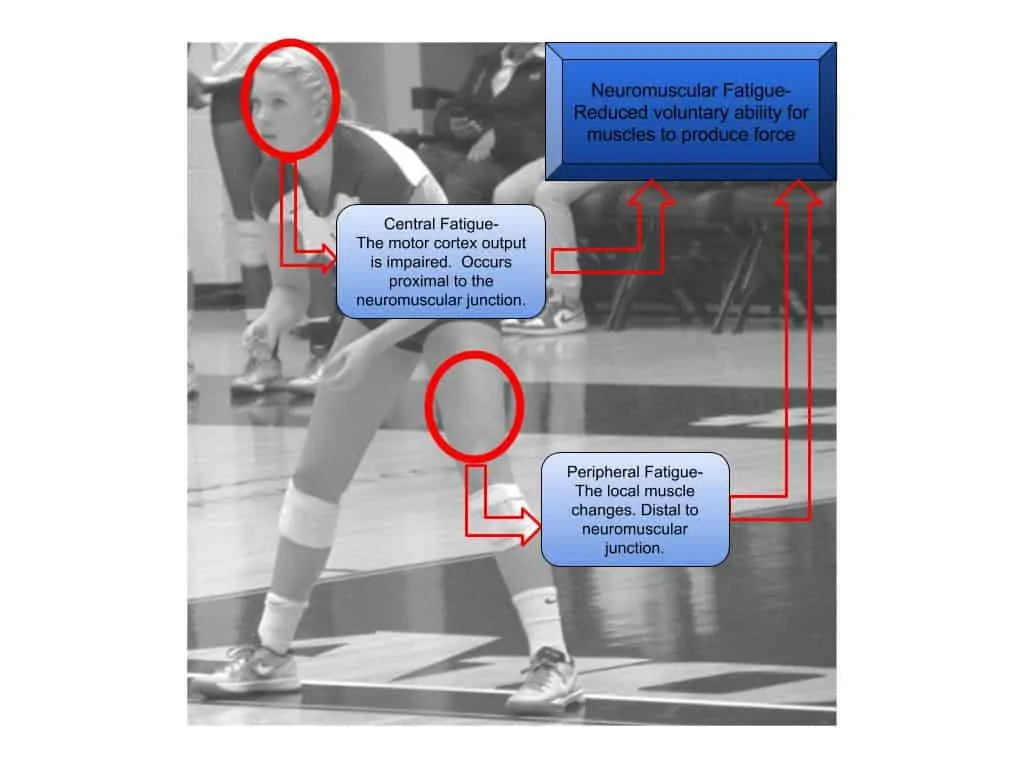
Ward S, Pearce AJ, Pietrosimone B, Bennell K, Clark R, Bryant AL. Neuromuscular deficits after peripheral joint injury: A neurophysiological hypothesis. Muscle Nerve. 2015;51(3):327-332. doi:10.1002/mus.24463.
Ageberg E, Björkman A, Rosén B, Roos EM. Principles of brain plasticity in improving sensorimotor function of the knee and leg in patients with anterior cruciate ligament injury: a double-blind randomized exploratory trial. BMC Musculoskelet Disord. 2012;13:68.
Gokeler A, Benjaminse A, Hewett TE, et al. Feedback Techniques to Target Functional Deficits Following Anterior Cruciate Ligament Reconstruction: Implications for Motor Control and Reduction of Second Injury Risk. Sports Med. 2013;43(11):1065-1074.
Grooms DR, Page SJ, Onate JA. Brain Activation for Knee Movement Measured Days Before Second Anterior Cruciate Ligament Injury: Neuroimaging in Musculoskeletal Medicine. J Athl Train. 2015;50(10):1005-1010.
Other articles on the knee
Physical Therapy Solutions for Knee Pain
Arthroscopic Partial Meniscectomy Surgery Vs Sham Surgery
Factors To Consider In Returning to Play
Physical Therapy Research: Update On The Knee And The Brain
Tuck Jump Assessment
Physical Therapy Exercises
Partner and Self Traction
Bracing, Taping, and Training Aids